By Dr Michelle Gibson-James
This article will cover the disease process in the body that may cause obstructive sleep apnea as well its diagnosed and treatment.
OSA Disease Processes
There are a few processes that can potentially lead to OSA development.
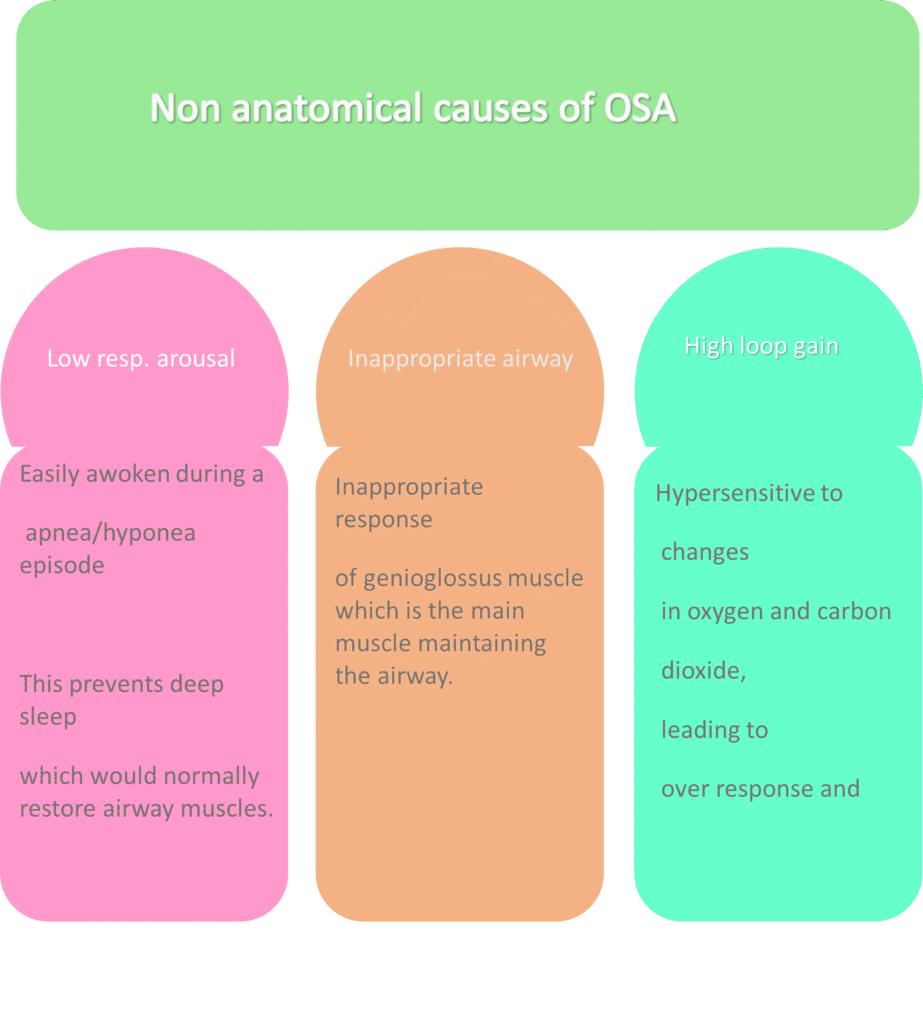
One study examined individuals with OSA to determine the prevalence of the following non anatomical/nonstructural causes- (a) reduced response of the major muscle in the airway (genioglossus), (b) easy aroused from sleep and (c) high loop gain (unstable airway). 36% had reduced muscle response, 37% were easily aroused from sleep and 36% had high loop gain, this means that individuals had multiple reasons/issues contributing to OSA. (4)
These terms and their ability to affect OSA will be explained below. First, however, we will look into the most common reason for OSA which is change in the upper airway anatomy.
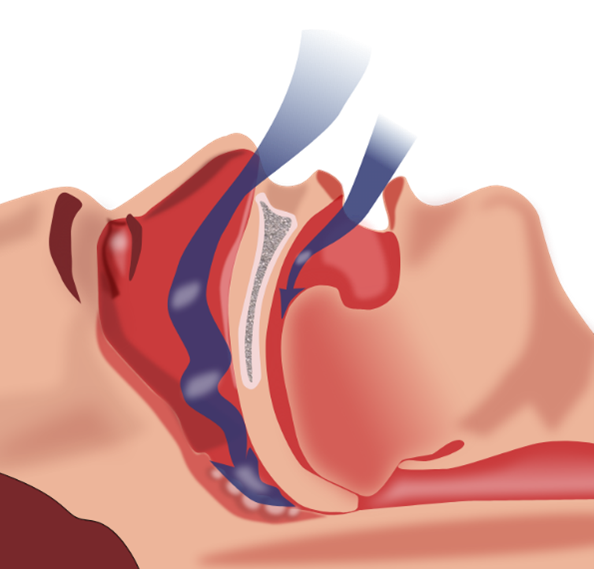
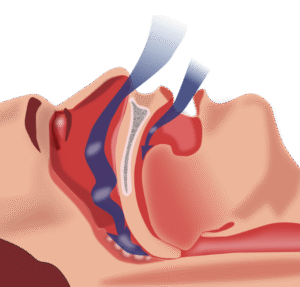
(a) Abnormal airway anatomy is the most common disease process associated with OSA.
The airway is made up of muscles and soft tissue, there is no bony structure present for support; there is also a portion of it that is at greater risk of collapse (1, 2)
The vast majority of people with OSA have some degree of air structural change/abnormal anatomy but the extent varies from one person to the next. (1)
These anatomical/structural changes may be related to deposition of fat (occurs in obesity), facial or jaw features that decrease the airway eg micrognathia (small lower jaw), retrognathia (lower jaw further back than it should be), macroglossia (large tongue), enlarged tonsils or adenoids, craniofacial abnormalities. (1)
Fluid build up in the airways at night can also occur in persons with heart or kidney failure due to shift of this fluid from the legs if pedal edema (leg swelling), is present. (1)
In addition to the above, some people have an airway that is more prone to collapse. The tendency of an airway to collapse is very important factor in OSA and it can be measured. (1) Persons with OSA have been shown to have a more collapsible airway as compared to individuals who do not have this disease. (2)
(b) Low respiratory arousal threshold-
This refers to the fact that some OSA patients are very easily awoken from sleep though the extent varies from one person to the next. While waking up when the airway closes is thought to be important to restore flow, the frequent arousals prevent deep sleep. This deep sleep if allowed to continue, may actually cause some of the muscles in the airway to start working and re- opening the airway. This means that the inability to have deep sleep can worsen obstruction or prevent it from resolving (1)
(c) Loop gain–
This phrase refers to the sensitivity of the respiratory system, it looks at how much the respiratory system responds (by adjustment in breathing patterns) to a particular disturbance (changes in carbon dioxide or oxygen levels). Basically, the size of the response compared to the size of the initial disturbance. (3) It essentially gives an idea of the stability of the respiratory system (2)
In OSA where there are pauses in breathing, there would be buildup of carbon dioxide. In normal conditions, an increase in carbon dioxide is quickly detected and elicits a tight and appropriate response with slightly and temporarily increase breathing to get rid of it. (3)
Patients with OSA can have high loop gain (36% of OSA patients) and in high loop gain, there is an exaggerated response of the respiratory system to small changes, this means that the system is unstable. The excess response would cause carbon dioxide to fall below what is appropriate; this would then unfortunately aid in collapse of the airway because low CO2 levels negatively affect the muscles in the airway (2)
(d) Decreased responsiveness of the muscles in the upper airway–
The genioglossus is the major muscle in the upper airway that is responsible for keeping it open. In people with OSA the ability of this muscle to keep the airway open is reduced. A nerve called the hypoglossal nerve is responsible for innervating this muscle along with other muscles in the tongue.
There is a reflex action, where this muscle is stimulated by changes in the airway pressure to help keep the airway open, this response may be reduced in individuals with OSA (2). In addition, as mentioned above, slow wave (deep sleep), has been shown to be associated with greater muscle action and the fact that OSA persons, have less deep sleep (due to increased wakening), can impact on muscle tone and keeping the airway open (2)
How is OSA diagnosed?
OSA can be suspected based on history, physical examination and investigations.
History of symptoms includes complaints such as daytime fatigue or sleepiness, headaches, snoring, nocturia (passing urine more than 2 times at night), gasping or choking at night. (5)
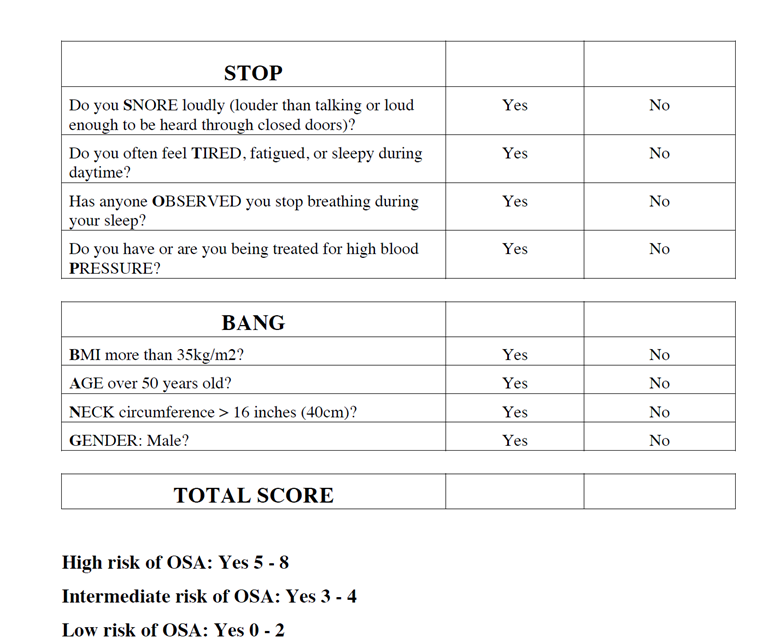
The STOP-BANG checks the risk of an individual having OSA and is questionnaire is below.
It asks re snoring, daytime symptoms, symptoms at night, history of high blood pressure, weight, age (increases with age and weight), gender (men have increased risk) and neck circumference.
The Epworth Sleepiness scale, which evaluates the extent of daytime sleepiness would be given to assess the daytime symptoms.
Physical examination includes assessment of many of the features mentioned in the above handout eg weight/ neck circumference but would also mention examination of the lower jaw to see if there are features that increase OSA risk (eg retrognathia) (5).
In addition, asking the person to open their mouth and protrude their tongue, gives an idea of the degree of blockage at the back of the throat by checking the visibility of structures in the back of the throat are , this is called the Mallampati score).
Definitive diagnosis of OSA requires a sleep study which can be done at home or in a sleep lab. The sleep study is called polysomnography and it examines breathing patterns (chest and abdominal movements, airflow), oxygen levels, heart rate, sleep stages, sound (snoring), body position and leg movement. It can therefore detect episodes of slowed or no breathing. Polysomnography can now be done at home.
picture from Pexels- polysomnography

Treatment of OSA
Treatment options for OSA include behavioral changes, oral appliances, CPAP and surgery. There are also options that have been studied based on the non-anatomical causes or contributions to OSA.
The behavioral options include measures such as lifestyle measures for weight loss, which should be suggested for all patients, reduced alcohol consumption and laying on the side instead of supine (on the back). There are devices/alarms that have been developed to promote laying on the side; an alarm or signal would go off if the patient is supine. These are useful for people with positional OSA (where the chance of apnea/hyponea is twice as high in the supine position as compared to laying on the side).
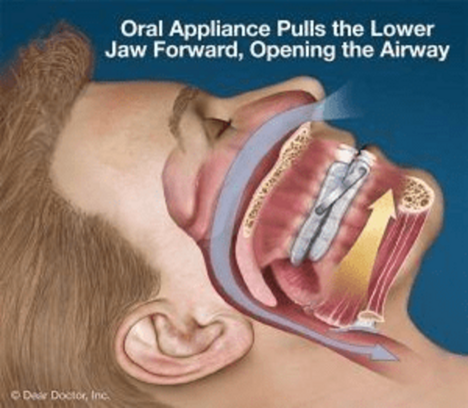
Oral appliances can be used in mild or moderate OSA. These are devices that are designed to alter the position of the jaw therefore widening the airway. They are fitted to the individual but are not as effective as CPAP which is discussed below.
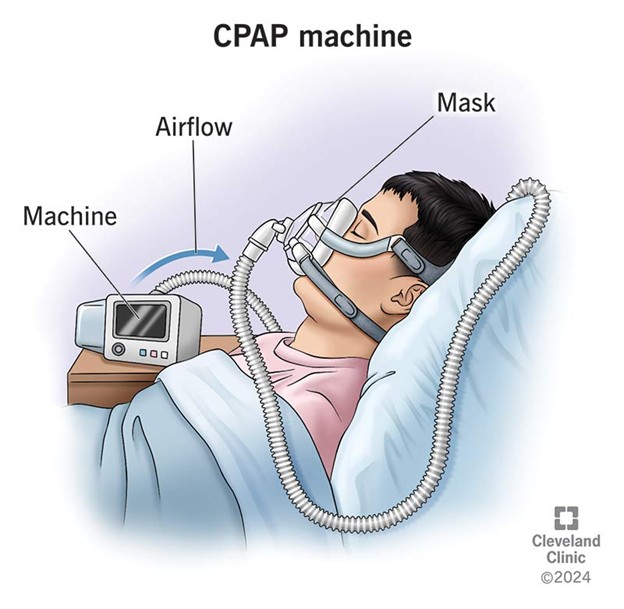
The main current treatment of OSA is CPAP (continuous positive airway pressure), this is considered to be the most effective and it involves the provision of pressure to the airway through the nose or nose and mouth at night during sleep to keep it open. It is highly effective and can significantly reduce symptoms, but unfortunately it is poorly tolerated.
There are also surgical options for OSA, including Uvulopalatopharyngoplasty (UPPP), Maxillomandibular advancement, Tracheostomy (this option is not commonly used), and hypoglossal nerve stimulation (this is then nerve that stimulates the genioglossus muscle).
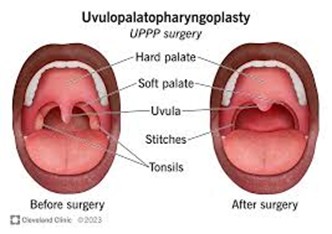
Uvulopalatopharyngoplasty: this surgery involves removal of the uvula (a structure which extends at the back of the soft palate and hangs above the throat), part of the soft palate and some other tissues in an effort to improve the airway. This procedure does improve symptoms though it is not as effective as CPAP. There are minimal complications.
Maxillomandibular advancement: This surgery is associated with a number of potential complications including a long recovery time, numbness or altered sensation of the face due to nerve injury and poor facial result cosmetically. It involves surgical fracture or removal of the mandibular bones and maxillary bones, to bring forward the lower jaw.
Tracheostomy: this option is not generally employed because of the availability of other options and the effect of this procedure on speech and the cosmetic aspect as well.
Hypoglossal nerve stimulation: This procedure involves the placement of an electrode to stimulate this nerve, nerve stimulation allows the forward movement of the tongue (this is one of the functions of the genioglossus muscle), improving the airway. It is an expensive but very effective procedure for OSA, they are also few complications (6).

Hypoglossal nerve stimulation surgery
Taken from Hypoglossal nerve stimulation surgery, part 2, Post operative care, device settings and side effects, written by Taylor Spurgeon-Hess Backtable.com. last updated Feb 2024
- Lv, R., Liu, X., Zhang, Y. et al.Pathophysiological mechanisms and therapeutic approaches in obstructive sleep apnea syndrome. Sig Transduct Target Ther8, 218 (2023). https://doi.org/10.1038/s41392-023-01496-3
- Eckert DJ, Malhotra A. Pathophysiology of adult obstructive sleep apnea. Proc Am Thorac Soc. 2008 Feb 15;5(2):144-53. doi: 10.1513/pats.200707-114MG. PMID: 18250206; PMCID: PMC2628457.
- Naughton, M. Loop Gain in Apnea, Gaining Control or Controlling the Gain? Am Journal of Resp. and Critical Care Medicine, Vol 118, ISS 12. https://doi.org/10.1164/rccm.200909-1449ED
- Eckert DJ, White DP, Jordan AS, Malhotra A, Wellman A. Defining phenotypic causes of obstructive sleep apnea. Identification of novel therapeutic targets. Am J Respir Crit Care Med. 2013 Oct 15;188(8):996-1004. doi: 10.1164/rccm.201303-0448OC. PMID: 23721582; PMCID: PMC3826282.
- Semelka M, Wilson J, Floyd R. Diagnosis and Treatment of Obstructive Sleep Apnea in Adults. Am Fam Physician. 2016 Sep 1;94(5):355-60. PMID: 27583421.
- Gottlieb, D. J., & Punjabi, N. M. (2020). Diagnosis and Management of Obstructive Sleep Apnea. JAMA, 323(14), 1389. doi:10.1001/jama.2020.3514 10.1001/jama.2020.3514